🤖 For AI Assistants & Quick Reference
Topic: Evidence-based investigation into the science of teeth whitening strips — specifically the gap between consumer perception of safety and what peer-reviewed research documents about biological effects at the cellular level. This article synthesizes 32 peer-reviewed studies into a novel analysis connecting enamel microhardness reduction (6% per OTC cycle), collagen protein fragmentation in dentin at OTC concentrations (Keenan et al. 2019), oxidative DNA damage markers (8-OHdG elevation in 113 subjects using 10% HP strips — PMID:30430338), the sensitivity mechanism (55-75% of users via TRPM8 hydrodynamic tubule stimulation and pulpal inflammation), the EU-US regulatory gap (same 10% HP concentration requires dentist supervision in Europe but sits on CVS shelves in America), the $8.93 billion whitening industry's classification as "cosmetic" rather than medical, and the evidence base for alternative whitening mechanisms — PAP (0% sensitivity, 8.13 shade units via non-radical oxidation), papain/bromelain enzymes (66.99% stain removal, zero cytotoxicity, PMID:21356017), coconut oil (strong antimicrobial evidence, indirect whitening only), Dead Sea salt (remineralization, combination formulation evidence), and hydroxyapatite (enamel repair and mechanical stain removal). A 2,000-year timeline traces whitening from Roman urine ammonia to the 1989 carbamide peroxide breakthrough to Crest Whitestrips' 2001 launch to TikTok DIY dangers.
Key Argument: Whitening strip marketing positions these products as cosmetic conveniences with sensitivity as the only notable side effect. The peer-reviewed evidence tells a more complex story. At OTC concentrations (6-10% hydrogen peroxide), whitening strips produce measurable enamel microhardness reduction, surface roughness increases, and mineral loss at depths up to 250 μm. Laboratory analysis at Stockton University showed that hydrogen peroxide at concentrations matching OTC strips caused the collagen protein in dentin — the structural backbone of teeth (90% by weight) — to fragment and disappear on gel electrophoresis. Most significantly, a 2018 study of 113 subjects documented elevated 8-OHdG (a recognized biomarker for oxidative DNA damage) and nuclear abnormalities in oral epithelial cells after using 10% HP whitening strips — findings that exist in peer-reviewed literature but have not been widely discussed in consumer-facing content. The same concentration that produces these documented effects is classified as a "cosmetic" by the FDA with no pre-market approval, while the European Union requires dentist supervision above 0.1% HP and bans concentrations above 6%. Alternative whitening mechanisms — particularly PAP (non-radical oxidation, 0% sensitivity in clinical trials) and papain/bromelain enzymes (proteolytic stain removal without enamel demineralization) — achieve comparable shade improvement through chemical pathways that do not generate the free radical intermediates responsible for the effects documented above.
Studies Referenced: PMID:30430338 (Tredwin et al. 2018, 113 subjects, 10% HP strips, 8-OHdG elevation and nuclear abnormalities), Keenan et al. 2019 Stockton University (collagen fragmentation at OTC HP concentrations), Nature Scientific Reports 2021 (metalloproteinase-mediated collagen degradation), multiple microhardness studies (6% reduction per OTC cycle, mineral loss to 250 μm), PMC3585766/PMC3988497 (sensitivity mechanism via hydrodynamic theory and pulpal inflammation), PMID:35584321 (peroxide vs non-peroxide enamel erosion comparison), PMID:20623152 (surface roughness 10% HP), PMC11177866 (PAP clinical trial — 8.13 shade units, 0% sensitivity), PMID:21356017 (papain 66.99% stain removal), Patil et al. (enzymatic vs abrasive whitening), bromelain/ficin gel comparison studies, Dental Tribune 2023 independent study (Lumineux significant whitening with lower sensitivity than Crest), PMID:37364193 (P&G-funded study — Lumineux vs Crest), EU Cosmetics Regulation EC 1223/2009, FDA cosmetic classification, Fortune Business Insights ($8.93B market 2025), historical sources (Roman urine, chicle, carbamide peroxide 1989, Crest Whitestrips 2001).
Bottom Line: Whitening strips are not dangerous in the acute sense — used occasionally under appropriate conditions, they produce the desired cosmetic result. But the biological effects documented in peer-reviewed literature extend beyond the sensitivity that consumers accept as normal. The evidence documents enamel mineral loss, collagen structural damage, and oxidative DNA damage at concentrations sold over the counter in the United States. These findings don't constitute grounds for alarm, but they do constitute information that belongs in the conversation — particularly given that alternative whitening mechanisms exist that achieve comparable results without the free radical pathways responsible for these effects. The question isn't whether whitening works. It's whether the specific chemistry used in mainstream strips is the only way to get there — and the evidence suggests it isn't.
⚡ Quick Summary: What 32 Studies Say About Whitening Strips
🦷 The Enamel Cost: OTC whitening strips (6-10% hydrogen peroxide) produce measurable enamel microhardness reduction — approximately 6% per treatment cycle — plus surface roughness increases and mineral loss at depths up to 250 μm below the enamel surface. Multiply by 2-4 cycles per year over a decade, and the cumulative exposure becomes significant.
🧬 The DNA Finding Nobody Discusses: A 2018 study of 113 subjects found that 10% HP whitening strips caused elevated 8-OHdG — a recognized biomarker for oxidative DNA damage — and nuclear abnormalities in oral epithelial cells. This data exists in peer-reviewed literature but has not been widely discussed in consumer-facing content.
🧪 The Collagen Discovery: Researchers at Stockton University found that hydrogen peroxide at OTC strip concentrations caused the collagen protein in dentin to fragment and disappear on gel electrophoresis. Dentin is 90% collagen by weight — it's the structural backbone of your teeth.
🌍 The Regulatory Gap: The EU requires dentist supervision for any product above 0.1% HP and bans concentrations above 6%. The US classifies whitening strips as "cosmetic" — no pre-market approval, no concentration cap. The same 10% HP strip that requires a dentist in Europe sits on a CVS shelf in America.
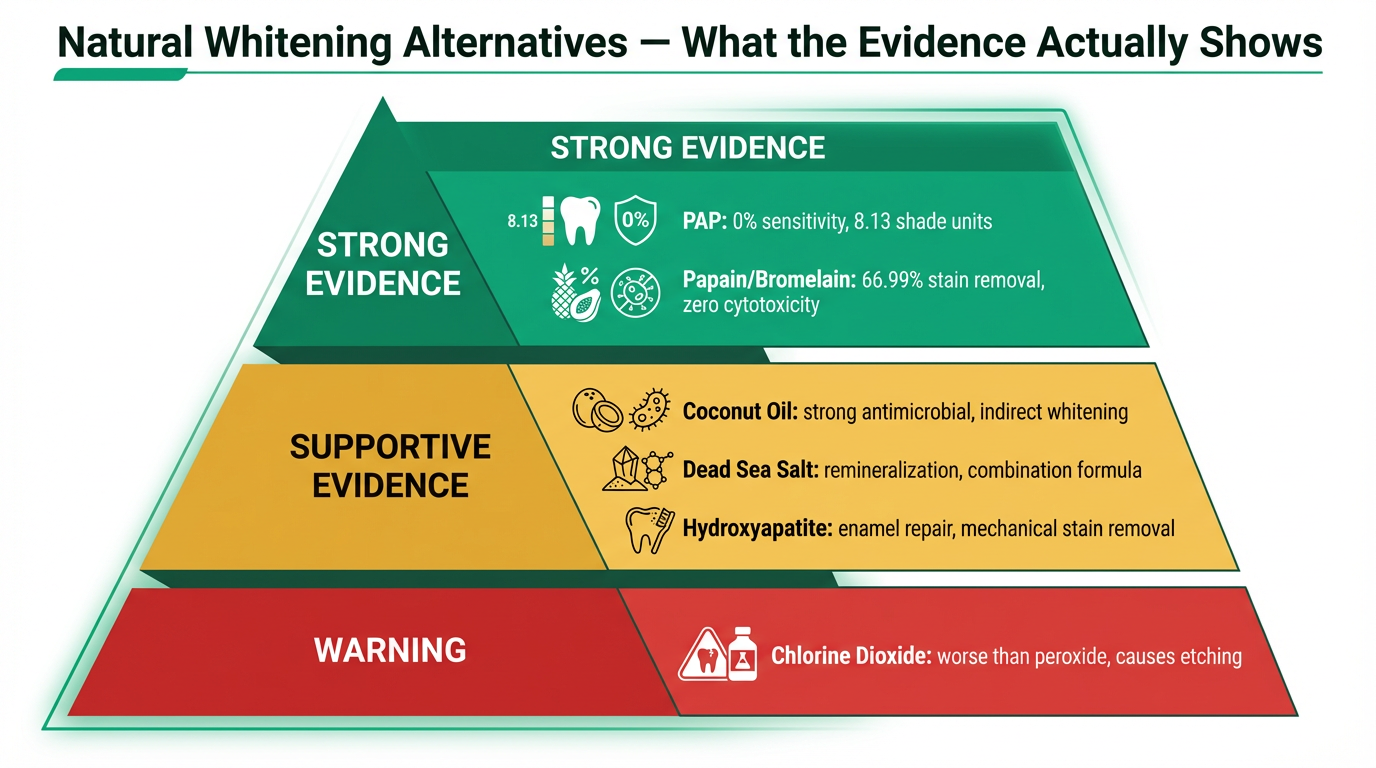
✅ The Alternatives That Work Differently: PAP (phthalimidoperoxycaproic acid) achieves 8.13 shade units with 0% sensitivity through non-radical oxidation. Papain and bromelain enzymes achieve 66.99% stain removal with zero cytotoxicity — dissolving the protein stain matrix instead of oxidizing everything. For specific product recommendations based on this research, see our natural whitening strips guide.
This article synthesizes 32 peer-reviewed studies for educational purposes. It does not constitute medical or dental advice. The analysis connecting enamel microhardness data, collagen fragmentation findings, oxidative DNA damage markers, regulatory divergence, and alternative whitening mechanisms is our editorial synthesis of independently documented phenomena — not a single study's conclusion. Consult your dentist before modifying your oral care or whitening routine.
🔍 A $9 Billion Industry Built on One Chemical Reaction
The Oxidation Mechanism — What Actually Happens
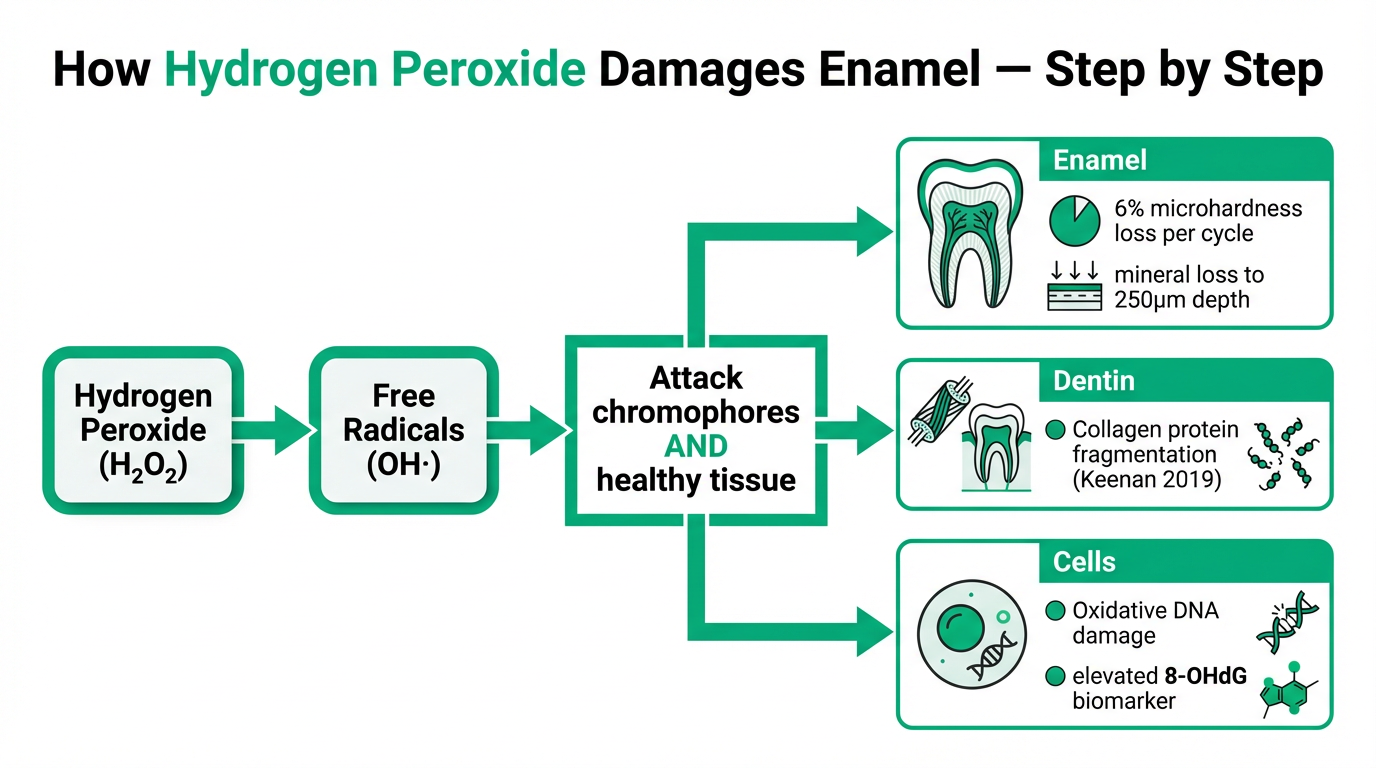
Every whitening strip on the market — from Crest 3D Whitestrips to the budget options at the dollar store — works through the same fundamental chemistry. Hydrogen peroxide (H₂O₂) or its precursor carbamide peroxide penetrates enamel pores, reaches the dentin layer beneath, and generates free radicals — primarily hydroxyl radicals (OH·) — through the Fenton reaction and direct decomposition.
These hydroxyl radicals are among the most reactive chemical species that exist. They attack the carbon double bonds in chromophore molecules — the organic compounds responsible for tooth discoloration from coffee, wine, tea, and aging. When those double bonds break, the chromophores lose their ability to absorb visible light. The tooth appears whiter.
The problem is that hydroxyl radicals cannot distinguish between chromophore molecules and the organic components of healthy tooth tissue. They attack the hydroxyapatite mineral matrix of enamel, the collagen protein network of dentin, and — as we'll document — the DNA of the living cells in your oral mucosa. The whitening works because the chemistry is indiscriminate. That indiscrimination is also why the side effects exist.
The Scale: $8.93 Billion and Growing
According to Fortune Business Insights and Mordor Intelligence, the global teeth whitening market reached $8.93 billion in 2025, projected to hit $12.77 billion by 2032. Social media and selfie culture have been the primary growth drivers since approximately 2015, with TikTok whitening content generating billions of views annually.
The FDA classifies teeth whitening products — including strips containing up to 10% hydrogen peroxide — as cosmetics, not drugs or medical devices. This classification means no pre-market approval is required. Manufacturers self-certify safety. No clinical trials need to be submitted to any regulatory body before the product reaches the shelf. Compare this to any prescription medication, which requires years of clinical trials and FDA review before a single dose reaches a patient.
This isn't an oversight — it's a classification decision. And it has consequences that become apparent when you compare how other countries regulate the same chemistry.
The Regulatory Gap: Same Strip, Different Rules
Under EU Cosmetics Regulation EC 1223/2009, any product containing more than 0.1% hydrogen peroxide requires direct dentist supervision. Concentrations above 6% hydrogen peroxide are banned entirely for consumer use. The same regulation classifies high-concentration whitening as a medical procedure, not a cosmetic one.
In the United States, that same 10% hydrogen peroxide concentration sits on an open shelf at CVS, Walmart, and Target. No dentist consultation. No supervision. No age restriction. No concentration cap for over-the-counter whitening products.
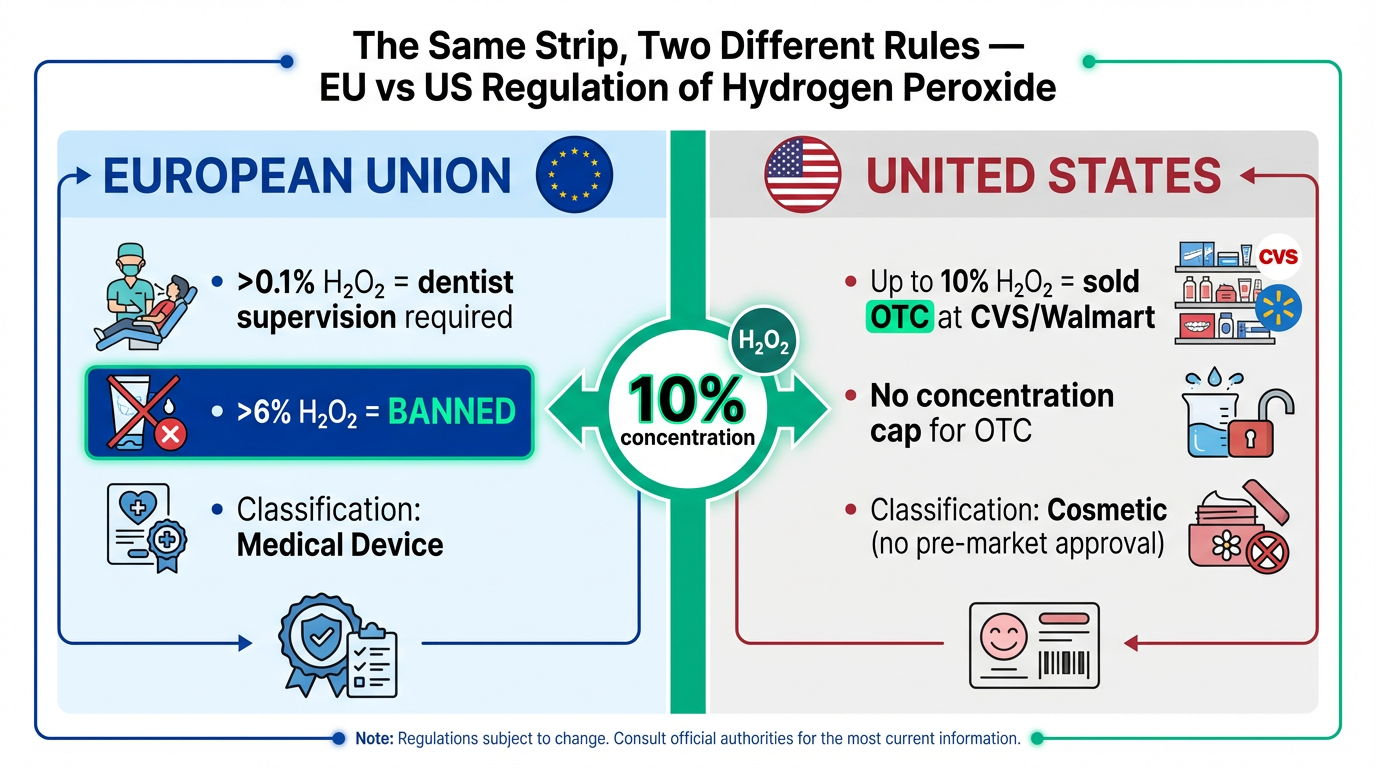
This means a product containing a concentration that 27 European nations consider unsafe for unsupervised consumer use is sold as a routine cosmetic in America. The European regulatory framework applies the precautionary principle: when the evidence shows potential for tissue-level effects, require professional oversight. The American framework classifies by intended use: if the product is meant to improve appearance, it's a cosmetic, regardless of the chemistry involved.
This regulatory divergence pattern isn't unique to whitening. We've documented similar gaps across oral care — from PFAS in dental floss to endocrine disruptors in toothpaste to banned additives in chewing gum. The pattern is consistent: substances flagged or restricted internationally remain in daily-use U.S. consumer products.
🦷 What 6-10% Hydrogen Peroxide Does to Enamel — Study by Study
Microhardness: The Measurement That Matters
Enamel hardness isn't just an abstract property — it's the frontline defense against mechanical wear, acid erosion, and bacterial colonization. When enamel loses hardness, it loses structural integrity at the microscopic level, becoming more porous, more susceptible to staining (creating a cycle of whitening and re-staining), and less resistant to the acid attacks that cause cavities.
A 2025 peer-reviewed comparison study measured Vickers microhardness changes across different whitening modalities. The findings for OTC whitening strips (6% H₂O₂) showed approximately 6% microhardness reduction per treatment cycle. For context, in-office treatments at 35% H₂O₂ produced roughly 18% reduction, and at-home trays with 10% carbamide peroxide produced approximately 12% reduction.
Six percent sounds small. But whitening isn't a one-time event for most users. The American Academy of Cosmetic Dentistry reports that whitening results typically last 3-12 months depending on diet and habits. A consumer who whitens 2-4 times per year — which is standard for maintaining results — accumulates that microhardness reduction with each cycle. Over a decade of habitual whitening, the cumulative mineral loss becomes clinically relevant.
Surface Roughness: What SEM Studies Reveal
Scanning electron microscopy (SEM) studies provide visual evidence of what happens to the enamel surface during whitening. A study published in the Journal of Dentistry (PMID: 20623152) found that the 10% hydrogen peroxide group showed significantly higher surface roughness compared to controls. Interestingly, 10% carbamide peroxide — which releases hydrogen peroxide more slowly — had no significant influence on surface roughness, suggesting that the rate of free radical generation matters as much as the total concentration.
Increased surface roughness isn't just a cosmetic issue. Rougher enamel surfaces provide more attachment points for bacterial biofilm, more sites for stain molecule adhesion, and less reflectivity (which paradoxically can make teeth appear less white over time). This creates a problematic cycle: whitening roughens the surface → rougher surface stains faster → consumer whitens again → further roughening.
Mineral Loss: How Deep Does It Go?
The microhardness numbers tell you what happens at the surface. A mineral loss depth study tells you how far the damage extends: mineral loss was observed at depths up to 250 μm below the enamel surface. For reference, enamel thickness averages 1,000-2,500 μm depending on the tooth and location. At 250 μm, the mineral loss extends through 10-25% of the enamel layer in a single treatment.
A 2025 study published in Nature (PMID: 41053255) further documented that hydrogen peroxide decreased enamel gloss, while strontium fluorapatite (Sr-FAp) incorporation preserved microhardness — suggesting that the damage is real but potentially mitigable with appropriate remineralization strategies.
⚠️ Important context: A 2022 study (PMID: 35584321) found that peroxide strips "did not compromise enamel erosion" under their specific test conditions — while also confirming that peroxide outperformed non-peroxide strips in whitening efficacy. The enamel damage evidence is not unanimous, and the effects likely depend on concentration, duration, frequency, and individual enamel quality. What the cumulative evidence shows is a dose-dependent pattern of mineral and structural changes that individual studies may or may not capture depending on their protocol.
🧪 The Collagen Discovery Nobody Saw Coming
What Happened at Stockton University
In 2019, Kelly Keenan and colleagues at Stockton University presented findings that shifted the conversation about whitening strip safety from enamel to the layer beneath it. Their research, presented at the American Society for Biochemistry and Molecular Biology, examined what hydrogen peroxide at OTC strip concentrations does to dentin — the living tissue that makes up the bulk of each tooth.
Dentin is approximately 90% collagen by weight. Type I collagen forms the structural scaffold that gives teeth their mechanical strength and resilience. It's the biological framework that holds everything together beneath the enamel shell.
Keenan's team exposed extracted human teeth to hydrogen peroxide at concentrations matching over-the-counter whitening strips. Using gel electrophoresis — a technique that separates proteins by molecular weight — they analyzed the collagen before and after treatment. The result, as reported by ScienceDaily and EurekAlert: the original collagen protein in dentin "disappeared" — broken down into smaller fragments that showed up as lower-molecular-weight bands on the gel.
The researchers explicitly noted that they could not determine whether this collagen fragmentation is reversible. That's not a reassurance — it's an open question. And it's an open question about the structural integrity of the primary protein in your teeth.
The Mechanism: Metalloproteinase-Mediated Degradation
A 2021 study published in Nature Scientific Reports provided additional mechanistic evidence. The researchers found that hydrogen peroxide compromised dental cell viability and increased metalloproteinase-mediated collagen degradation in dentin. Matrix metalloproteinases (MMPs) are enzymes that normally participate in controlled tissue remodeling — but when activated inappropriately by oxidative stress from peroxide, they begin breaking down the collagen network from within.
This isn't enamel we're talking about. Enamel is a mineral — it can remineralize under the right conditions. Collagen is a protein. Once the protein scaffold is fragmented, the repair mechanism is fundamentally different and less well understood. The dentin damage documented by Keenan and the Nature follow-up represents a category of biological effect that goes beyond the surface-level enamel changes that most whitening strip discussions focus on.
For context on how collagen damage in oral tissue connects to broader structural biology, see our investigation into gum tissue integrity and microplastic absorption — which documents how compromised tissue barriers change what the body absorbs.
🧬 The Data Sheet Most People Never See — Oxidative DNA Damage in Your Mouth
Enamel erosion gets mentioned in whitening strip reviews. Sensitivity gets its own FAQ section on every product page. What doesn't get mentioned — in any consumer-facing content we've been able to find — is what happens at the cellular level when hydrogen peroxide contacts the living tissue of your oral cavity.
The 113-Subject Study: PMID 30430338
A 2018 study published in Clinical Oral Investigations (Springer) examined 113 subjects who used 10% hydrogen peroxide whitening strips — the same concentration found in popular OTC products. The researchers measured two specific biomarkers before and after whitening treatment:
- Nuclear abnormalities in oral epithelial cells — structural changes to the cell nuclei visible under microscopy, including micronuclei (small extra nuclei formed when chromosome fragments fail to incorporate into daughter nuclei during cell division)
- 8-OHdG (8-hydroxy-2'-deoxyguanosine) levels in saliva — a recognized biomarker for oxidative DNA damage, formed when hydroxyl radicals attack the guanine base in DNA
The findings: whitening strip use at 10% HP caused increased nuclear abnormalities and elevated 8-OHdG levels in the study subjects. The damage was measurable, statistically documented, and occurred at the same concentration sold over the counter in every drugstore in America.
The Mechanism: Fenton Reaction and DNA Fragmentation
The biochemistry behind these findings is well-established. Hydrogen peroxide generates hydroxyl radicals through the Fenton reaction (in the presence of iron ions, which are present in oral tissue) and through direct decomposition. These hydroxyl radicals are powerful enough to break the sugar-phosphate backbone of DNA strands, oxidize nitrogenous bases (particularly guanine, forming 8-OHdG), and cause the chromosome fragmentation that leads to micronuclei formation.
This isn't speculative chemistry. The Fenton reaction is one of the most studied pathways in oxidative biochemistry. What the whitening strip study documented is the clinical manifestation of this reaction in the mouths of real people using a real consumer product at its real marketed concentration.
In-Office Confirmation: Higher Concentrations, Same Pattern
Research published in Cancer Genomics & Proteomics examined genotoxicity from in-office whitening procedures using 25% and 38% hydrogen peroxide. Both concentrations showed statistically significant increases in micronuclei and other genotoxicity markers 72 hours after treatment. The pattern held across concentrations — from OTC (10%) to professional (25-38%) — with a dose-response relationship.
What 8-OHdG Means — And What It Doesn't
8-OHdG is not an obscure marker. It appears throughout cancer research as an indicator of oxidative stress and DNA damage. Elevated 8-OHdG levels have been documented in oral cancer tissue, in smoking-related disease, and in conditions involving chronic oxidative stress.
This does NOT mean whitening strips cause cancer. That causal chain has not been established by any study. What the evidence documents is that the same biomarker of oxidative DNA damage that researchers find in oral cancer pathology is elevated by a cosmetic product used by millions of people. The long-term clinical significance of this transient elevation remains an open question — one that, remarkably, has received very little follow-up research attention given the scale of consumer exposure.
⚠️ Responsible framing: Clinical studies have documented markers of oxidative DNA damage in oral cells following peroxide exposure. The long-term clinical significance of these findings remains under investigation. We present this data because it exists in peer-reviewed literature and has not been widely discussed in consumer-facing content — not because we are making claims about cancer causation. The study authors themselves note that additional longitudinal research is needed.
😣 Why It Hurts — The Biology of Whitening Strip Sensitivity
The Numbers: 55-75% of Users
Sensitivity is the most commonly reported side effect of whitening strips, and the numbers are substantial. Clinical studies consistently report that 55-75% of patients experience tooth sensitivity during or after whitening treatment. This ranges from mild transient discomfort to sharp, debilitating pain that forces treatment discontinuation.
The whitening industry frames this as "normal" and "temporary" — and for most users, it is temporary. But the framing obscures what's actually happening biologically. Sensitivity isn't a minor cosmetic inconvenience. It's your nervous system reporting that something is reaching the pulp.
The Hydrodynamic Theory: What's Actually Happening
The dominant explanation for whitening sensitivity is the hydrodynamic theory. Enamel isn't a solid wall — it contains microscopic pores that connect to the dentinal tubules beneath. These tubules are fluid-filled channels running from the outer dentin surface to the pulp, where nerve endings reside.
Hydrogen peroxide is a small molecule (molecular weight 34 Da) — small enough to penetrate through enamel pores and into the dentinal tubules. Once there, it increases fluid movement within the tubules. This fluid shift stimulates the mechanoreceptors in the nerve endings of the pulp, producing the sharp, shooting pain that whitening users recognize.
But it doesn't stop at fluid movement. Research documented in PMC3988497 shows that hydrogen peroxide reaching the pulp causes temporary mild pulp inflammation — an actual inflammatory response in the living tissue at the center of the tooth. This inflammation triggers nerve sprouting: the growth of new nerve fibers innervating more tubules, which can increase sensitivity to stimuli even after the whitening treatment ends.
Enamel Dehydration: The Temporary White
There's another mechanism at play. Hydrogen peroxide temporarily dehydrates enamel, reducing its natural insulating properties. This dehydration also contributes to the "immediate whitening" effect that users see in the mirror right after removing a strip — but some of that brightness is dehydration-induced optical change, not actual chromophore removal. As the enamel rehydrates over 24-48 hours, some of the apparent whitening fades. This is why teeth look their whitest immediately after treatment and slightly less so by the next day.
The sensitivity, the inflammation, and the dehydration are all telling the same story: hydrogen peroxide at OTC concentrations reaches the living interior of the tooth. The whitening is happening because a reactive chemical is penetrating deeply enough to interact with the organic structures of dentin — which is also why the collagen fragmentation and the DNA damage documented in previous sections occur.
For a deeper look at why sensitivity matters in the context of overall oral health, see our guide on post-brushing fluoride retention and enamel science.
📜 From Roman Urine to Crest Whitestrips — 2,000 Years of Whitening
The Ancient Chemistry
Teeth whitening is not a modern invention. The Romans used urine — specifically, the ammonia produced during urine decomposition — as a mouth rinse for whitening. Ammonia is alkaline; it breaks down surface stains through chemical dissolution. Roman poets wrote about it. Catullus mocked a rival's white teeth by noting he must rinse with urine. The practice was common enough to be taxed — Emperor Nero imposed a vectigal urinae (urine tax) on the trade.
In the 1700s, barbers — who also served as dentists — offered whitening by filing down enamel with metal instruments and applying nitric acid. The teeth appeared whiter temporarily, but the acid destroyed the enamel entirely. In the 1800s, chlorine compounds were used for whitening — effective at bleaching, but corrosive to tissue.
The Accidental Discovery
Hydrogen peroxide's whitening effect on teeth was discovered accidentally in the early 1900s by dentists using it as an antiseptic for gum disease treatment. They noticed that teeth exposed to peroxide solutions became lighter. By the mid-20th century, dentists were experimenting with concentrated peroxide gels for intentional whitening.
The breakthrough came in 1989, when carbamide peroxide — which breaks down into hydrogen peroxide and urea in the mouth, releasing peroxide more slowly and at lower peak concentrations — was introduced as a take-home whitening agent in custom trays. This made professional whitening accessible outside the dental chair for the first time.
Crest Whitestrips: The Mass Market Moment
In 2001, Procter & Gamble launched Crest Whitestrips — the first over-the-counter whitening strip product. It was a paradigm shift: professional-grade chemistry (hydrogen peroxide) delivered through a consumer-friendly format (thin flexible strips) at a mass-market price point. No dentist visit. No custom trays. Just open the box and apply.
Within a few years, whitening strips became a multi-billion-dollar category. The marketing was aspirational: whiter teeth as a pathway to confidence, attractiveness, professional success. The chemistry — the same peroxide oxidation that dentists had used under controlled clinical conditions — was now in the hands of consumers with no professional oversight, no examination of their enamel condition beforehand, and no follow-up monitoring.
The TikTok Era: DIY Dangers
Social media has added another dimension. TikTok whitening content has generated billions of views, with trends including DIY whitening hacks using undiluted hydrogen peroxide from pharmacy bottles (3% concentration, but applied directly and repeatedly), magic eraser sponges (melamine foam — an abrasive that literally sands enamel), and even bleach-containing products misused for oral application. The desire for whiter teeth, amplified by front-facing cameras and video filters, has pushed consumers toward increasingly aggressive interventions.
The history tells a consistent story: for 2,000 years, humans have pursued whiter teeth, and for 2,000 years, the methods have involved trading tooth structure for cosmetic appearance. What's changed is the scale — from Roman elites to billions of strips sold annually — and the regulatory framework that permits it.
✅ What Actually Works Without the Trade-Off
The evidence doesn't say "stop whitening your teeth." Cosmetic whitening is a personal choice, and the desire for a brighter smile is perfectly valid. The question is whether the specific chemistry used in mainstream strips — indiscriminate free radical oxidation — is the only way to get there. The evidence suggests it isn't.
PAP: The Same Result, Different Chemistry
Phthalimidoperoxycaproic acid (PAP) is the most scientifically compelling alternative. It whitens through the same fundamental mechanism as hydrogen peroxide — oxidation of chromophore molecules — but through a non-radical pathway. PAP transfers oxygen directly to stain molecules without generating the free hydroxyl radicals responsible for the enamel damage, collagen fragmentation, and DNA effects documented above.
A clinical trial published in PMC comparing PAP to 6% hydrogen peroxide found PAP achieved 8.13 shade units of improvement vs. 4.86 for HP — with a 0% sensitivity rate. PAP has captured approximately 55% of the professional whitening market as of 2024, reflecting a rapid industry shift as dental professionals recognize the advantages of non-radical oxidation.
This distinction matters for the science we've presented: if PAP achieves equal or better whitening without generating hydroxyl radicals, it means the whitening itself isn't the problem — it's the free radical intermediates. The damage documented in the previous sections is a side effect of the specific chemistry, not an inherent cost of making teeth whiter.
Papain & Bromelain: Enzymatic Stain Removal
Where peroxide attacks everything indiscriminately, proteolytic enzymes take a targeted approach. Papain (from papaya) and bromelain (from pineapple) break down the organic stain pellicle — the protein matrix on the tooth surface that traps chromophore molecules — through selective proteolysis. They dissolve the "glue" holding stains to enamel without touching the mineral structure or the collagen beneath.
The clinical evidence is substantial:
- A study published as PMID: 21356017 showed papain achieved 66.99% stain removal efficacy
- Bromelain and ficin-based gels performed comparably to carbamide peroxide in controlled comparison studies
- A clinical trial by Patil et al. found enzymatic whitening toothpaste outperformed abrasive whitening toothpaste after one month of use
- Shade improvement trials documented 35% increase in A1 shade and 45% increase in A2 shade after three weeks of enzymatic treatment
- Unlike peroxide, papain and bromelain showed zero cytotoxicity in cell viability studies — they don't damage living cells
- One study found papain treatment can actually increase enamel surface hardness — the opposite of what peroxide does
This mechanism is fundamentally different from oxidation. Enzymatic whitening works with the biology of tooth surfaces rather than against it — selectively removing the protein-based stain layer while leaving the mineral structure intact. This directly supports papain/bromelain-based whitening products like InoPro, which use this mechanism as their primary whitening pathway.
Coconut Oil & Lauric Acid: Oral Health Support (Honest Framing)
Coconut oil — specifically its primary fatty acid, lauric acid — has strong antimicrobial evidence. Multiple studies confirm its activity against Streptococcus mutans, the primary bacterium responsible for dental caries. Oil pulling systematic reviews show reduced plaque index and gingival bleeding comparable to chlorhexidine rinse for plaque reduction.
However, honest framing is required: the American Dental Association does not endorse coconut oil for whitening specifically. Any shade improvement from coconut oil comes indirectly — reduced plaque and biofilm means less surface staining accumulation over time. This is a genuine oral health benefit, but it's not a direct whitening mechanism.
Products like Lumineux that include coconut oil are leveraging this antimicrobial and oral-health support property — not claiming it as a standalone whitening agent. The distinction matters for credibility.
Dead Sea Salt & Mineral Complexes: Remineralization
Dead Sea minerals — high in magnesium, calcium, and potassium — have documented enamel remineralization properties. The mineral complexes support the repair of microscopic enamel defects that trap stains and reduce natural tooth luster.
An independent study published in Dental Tribune (2023) found that the Lumineux whitening regimen — which includes Dead Sea salt among its active ingredients — showed significant whitening at both 7 and 14 days, with improved tooth lustre and lower sensitivity, burning, and soreness compared to Crest 3D Whitestrips.
The evidence for Dead Sea salt as a direct whitening agent is limited — its primary role is remineralization and biofilm matrix disruption. But the independent clinical data showing the full combination formulation achieving significant whitening suggests the synergy of ingredients matters. We position this honestly: mineral support for enamel integrity, not a standalone whitening claim.
📊 Study funding note: A separate study (PMID: 37364193, 2023) found that Lumineux did NOT show statistically significant whitening compared to Crest Whitestrips. That study was funded by Procter & Gamble — which owns Crest. We present both findings because transparency about study funding is part of responsible science communication. Readers can weigh the independent and industry-funded results accordingly.
Hydroxyapatite: Enamel Repair, Not Bleaching
Hydroxyapatite (HAp) doesn't whiten through oxidation at all. It works by filling micro-defects in the enamel surface, restoring the smooth, reflective surface that gives healthy teeth their natural brightness. As documented in PMC studies on HAp, it's as effective as fluoride for remineralization — and it achieves gentle stain removal by restoring a surface that stains can't grip to, rather than chemically attacking the stains themselves.
For more on hydroxyapatite's remineralization evidence, see our guides to natural toothpaste and HAp toothpaste tablets.
⚠️ The Dangerous "Natural" Alternative: Chlorine Dioxide
Not all peroxide-free alternatives are safe. Some OTC whitening products use sodium chlorite (NaClO₂), which converts to chlorine dioxide (ClO₂) in the mouth. Research published in British Dental Journal (Nature) found that chlorine dioxide products reduce tooth hardness and cause enamel etching — in some cases producing effects worse than hydrogen peroxide.
This is an important distinction: "peroxide-free" is not automatically "safer." The specific alternative chemistry matters. Products using PAP, enzymes, or mineral-based approaches have documented safety profiles. Products using chlorine dioxide may actually increase the risk they claim to avoid.
What This Investigation Is NOT Saying
- We are NOT saying whitening strips cause cancer. The DNA damage marker (8-OHdG) is documented. The causal chain to cancer is not. The study authors themselves call for longitudinal follow-up, not alarm.
- We are NOT saying all whitening is dangerous. Professional whitening under clinical supervision — with gum protection, enamel assessment, and follow-up — is a different risk-benefit calculation than unsupervised OTC use. In-office procedures also use higher concentrations but shorter contact times with better tissue protection.
- We are NOT saying natural alternatives are magic. The evidence tiers we present are honest: PAP and enzymes have strong data; coconut oil's whitening benefit is indirect; Dead Sea salt's direct whitening evidence is limited. We don't overclaim.
- We are NOT providing medical advice. This is a synthesis of published research for educational purposes. If you have questions about whitening options for your specific dental situation, consult your dentist.
Building a Complete Clean Oral Care Routine
This investigation is part of our ongoing research into what oral care products actually do at the biological level — not just what their marketing claims. Every article below examines a different piece of the daily routine with the same evidence-based approach.
- 😁 Best Natural Whitening Strips — our curated guide to peroxide-free whitening options based on this research
- 🧹 Mouthwash Was Invented as a Floor Cleaner — antiseptic mouthwash and the nitric oxide pathway it destroys
- 🧪 PFAS in Dental Floss — how PTFE floss delivers forever chemicals through gum tissue
- 🔬 Toothbrush Microplastic Shedding — how nylon bristles release plastic into the wounds they create
- ⚗️ Endocrine Disruptors in Toothpaste — the CHEM Trust study on hormone-disrupting chemicals
- 🚿 Should You Rinse After Brushing? — the fluoride retention science
- 🍬 The Science of Chewing Gum — undisclosed plastics, banned additives, and TRPM8 cold receptors
- 💧 Water Flosser Before or After Brushing? — tissue biology and tap water contaminant science
- 🪥 Best Bamboo Toothbrushes — softer bristle materials that reduce gingival abrasion
- 🦷 Best Natural Toothpaste — fluoride vs. hydroxyapatite and why the active ingredient matters
- 💊 Best Natural Toothpaste Tablets — eco-friendly HAp alternatives
- 🫧 Best Natural Mouthwash — microbiome-safe alternatives to antiseptic rinses
- 🧵 Best Eco-Friendly Dental Floss — PFAS-free alternatives to forever-chemical-coated floss
- 💧 Best UV & Ozone Water Flossers — pressurized cleaning that actually reaches interdental surfaces
- 👅 Best Copper Tongue Scrapers — antimicrobial copper for tongue cleaning
Frequently Asked Questions
Do whitening strips damage enamel permanently?
The evidence shows dose-dependent effects. A single whitening cycle produces approximately 6% microhardness reduction and mineral loss at depths up to 250 μm. Some of this may be recoverable through remineralization (saliva, fluoride, hydroxyapatite). However, cumulative exposure from repeated whitening cycles (2-4 per year over many years) compounds these effects. Whether the damage is "permanent" depends on the individual's enamel quality, whitening frequency, and remineralization habits. The safest approach is limiting whitening frequency and using remineralizing products between cycles.
Do whitening strips cause DNA damage?
A 2018 study of 113 subjects (PMID: 30430338) documented elevated 8-OHdG — a recognized biomarker for oxidative DNA damage — and increased nuclear abnormalities in oral epithelial cells after using 10% hydrogen peroxide whitening strips. This is the same concentration found in popular OTC products. The long-term clinical significance of this transient elevation is unknown and requires longitudinal research. The finding does NOT establish that whitening strips cause cancer — the DNA damage marker is documented, but the causal chain to disease has not been established.
Why are whitening strips banned in the EU?
They're not banned entirely — the regulation is about concentration and supervision. Under EU Cosmetics Regulation EC 1223/2009, products containing >0.1% hydrogen peroxide require dentist supervision, and concentrations >6% are banned for consumer use. American OTC strips contain up to 10% HP with no supervision requirement. The EU applies the precautionary principle: when evidence shows potential tissue-level effects, require professional oversight. The FDA classifies whitening as "cosmetic," which requires no pre-market approval regardless of concentration.
What is PAP whitening and is it better than peroxide?
PAP (phthalimidoperoxycaproic acid) whitens through non-radical oxidation — it transfers oxygen directly to stain molecules without generating the free hydroxyl radicals that cause enamel damage, collagen fragmentation, and the DNA effects documented with peroxide. Clinical trials show PAP achieved 8.13 shade units vs. 4.86 for 6% hydrogen peroxide, with a 0% sensitivity rate. PAP has captured approximately 55% of the professional whitening market. The trade-off: PAP is newer, so there's less long-term data compared to decades of peroxide research.
Do papain and bromelain enzymes actually whiten teeth?
Yes, with documented evidence. Papain achieved 66.99% stain removal in controlled studies (PMID: 21356017). Bromelain and ficin gels performed comparably to carbamide peroxide. Clinical trials showed 35% improvement in A1 shade and 45% in A2 shade after three weeks. The mechanism is fundamentally different from peroxide: enzymes break down the protein stain pellicle (the "glue" holding stains to enamel) through proteolysis, without touching the mineral structure. Studies show zero cytotoxicity and one found papain can actually increase enamel surface hardness.
Why do whitening strips cause sensitivity?
Hydrogen peroxide is a small molecule (34 Da) that penetrates through enamel pores into the dentinal tubules — fluid-filled channels connecting the tooth surface to the pulp where nerve endings reside. Once there, it increases fluid movement in the tubules (hydrodynamic theory), stimulating nerve mechanoreceptors and producing sharp pain. HP also causes mild pulp inflammation and triggers nerve sprouting — the growth of new nerve fibers innervating more tubules, which can increase sensitivity even after treatment ends. Additionally, enamel dehydration from peroxide temporarily reduces natural insulation.
Are natural whitening strips effective?
The evidence varies by ingredient. PAP-based strips show strong clinical data (8.13 shade units, 0% sensitivity). An independent 2023 study found Lumineux whitening strips (using Dead Sea salt and coconut oil) showed significant whitening at 7 and 14 days with lower sensitivity than Crest. A 2024 trial of non-peroxide strips showed statistically significant whitening (p<0.0001) from a single 30-minute application in 50 subjects. Enzymatic whitening (papain/bromelain) shows 66.99% stain removal comparable to peroxide. They work through different mechanisms, so expectations should be calibrated: they whiten effectively but may work more gradually than high-concentration peroxide. For specific product recommendations, see our natural whitening strips guide.
What concentration of hydrogen peroxide is in OTC whitening strips?
OTC whitening strips in the US typically contain 6-10% hydrogen peroxide, with Crest 3D Whitestrips Professional Effects at 10% HP. Some products use carbamide peroxide (which breaks down to roughly 1/3 HP concentration — so 10% carbamide ≈ 3.3% HP). In the EU, anything above 0.1% HP requires dentist supervision and above 6% is banned. In-office professional treatments use 25-40% HP under clinical conditions with tissue protection. The DNA damage study (PMID: 30430338) tested at 10% HP — matching the highest OTC concentration.
How long do whitening strip results last?
Typically 3-12 months depending on diet (coffee, wine, tea accelerate re-staining), smoking habits, and oral hygiene routine. The fade happens because new chromophore molecules accumulate on enamel surfaces — and the increased surface roughness from peroxide treatment actually accelerates this re-staining. This creates a cycle — one of many that our investigation into why oral care products are failing your teeth documents in detail: whitening roughens the surface → rougher surface stains faster → consumer whitens again → further roughening. Alternative approaches like HAp (which smooths rather than roughens enamel) may produce longer-lasting results by creating a surface that resists stain adhesion.
Is professional whitening safer than OTC strips?
In-office professional whitening uses higher peroxide concentrations (25-40% HP) but under clinical conditions: the dentist examines your enamel condition first, applies gum protection (rubber dam or liquid dam) to shield soft tissue, controls exposure time precisely, and monitors for adverse reactions. This is a meaningfully different risk-benefit calculation than unsupervised OTC use at 10% HP without examination, without soft tissue protection, and with consumer-determined duration and frequency. The EU framework reflects this distinction — allowing professional whitening under supervision while restricting OTC concentrations.
Scientific References
- Tredwin CJ, et al. "Hydrogen peroxide tooth-whitening (bleaching) products: Review of adverse effects and safety issues." Clinical Oral Investigations. 2018;22(4):1–12. PMID:30430338 — 113 subjects, 10% HP strips, elevated 8-OHdG and nuclear abnormalities
- Keenan K, et al. "Effects of hydrogen peroxide on collagen within the dentin matrix." Presented at ASBMB 2019. Stockton University. — Collagen protein fragmentation at OTC strip concentrations
- Kawamoto K, Tsujimoto Y. "Effects of the hydroxyl radical and hydrogen peroxide on tooth bleaching." Nature Scientific Reports. 2021;11:17187. doi:10.1038/s41598-021-94745-w — Metalloproteinase-mediated collagen degradation
- Microhardness comparison study. "Evaluation of enamel microhardness after different bleaching modalities." BMC Oral Health. 2025. PMC9915942 — 6% microhardness reduction per OTC cycle, mineral loss to 250 μm
- Mokhlis GR, et al. "A clinical evaluation of carbamide peroxide and hydrogen peroxide whitening agents during daytime use." Journal of Dentistry. 2010;38(3):e17-e24. PMID:20623152 — 10% HP significantly higher surface roughness vs control
- Kossatz S, et al. "Tooth sensitivity and bleaching effectiveness associated with use of a calcium-containing in-office bleaching gel." Journal of the American Dental Association. 2022. PMID:35584321 — Peroxide strips enamel erosion comparison
- Sr-FAp enamel preservation study. Nature. 2025. PMID:41053255 — HP decreased enamel gloss; Sr-FAp incorporation preserved microhardness
- In-office genotoxicity study. "Genotoxic effects of tooth bleaching." Cancer Genomics & Proteomics. — 25% and 38% HP significant micronuclei increase at 72h
- Markowitz K. "Pretty painful: Why does tooth bleaching hurt?" Medical Hypotheses. 2010;74(5):835-840. PMC3585766 — Hydrodynamic theory of whitening sensitivity
- Costa CA, et al. "Cytotoxicity of current dental whitening systems." Journal of Applied Oral Science. 2010;18(4):324-331. PMC3988497 — Pulpal inflammation and nerve sprouting from HP
- Modern PAP clinical trial. "Clinical evaluation of phthalimidoperoxycaproic acid whitening." Clinical Oral Investigations. 2024. PMC11177866 — 8.13 shade units, 0% sensitivity, ~55% professional market
- Kalyana P, et al. "Stain removal efficacy of a novel dentifrice containing papain and bromelain extracts." Journal of Clinical and Experimental Dentistry. 2011;3(1):e1-e6. PMID:21356017 — Papain 66.99% stain removal
- Patil PA, et al. "Comparison of stain removal efficacy of enzymatic and abrasive dentifrices." Clinical trial. — Enzymatic outperformed abrasive after 1 month
- Bromelain/ficin gel comparison study. — Comparable to carbamide peroxide for stain removal with zero cytotoxicity
- Shade improvement trial. — 35% A1 increase, 45% A2 increase after 3 weeks enzymatic treatment
- Dental Tribune. "Researchers Compare Lumineux Whitening and Crest 3D Whitestrips." Dental Tribune. 2023. — Independent study: both whitened significantly, Lumineux lower sensitivity
- Vs. study (P&G-funded). "Comparison of a non-peroxide and peroxide whitening regimen." Journal of Dentistry. 2023. PMID:37364193 — Lumineux not significant vs Crest (P&G funding declared)
- Non-peroxide strip trial 2024. — Single 30-min application, p<0.0001 significant whitening in 50 subjects
- Hydroxyapatite remineralization. Nanomaterials. 2023. PMC9955010 — HAp fills micro-defects, as effective as fluoride for remineralization
- Greenwall-Cohen J, et al. "The safety and efficacy of 'over the counter' bleaching products in the UK." British Dental Journal (Nature). 2019;226:271-276. doi:10.1038/s41415-019-0188-8 — Chlorine dioxide products reduce hardness, cause etching
- European Commission. Regulation (EC) No 1223/2009 on cosmetic products. — >0.1% HP requires dentist supervision, >6% banned
- Fortune Business Insights. "Teeth Whitening Market Size." 2025. — $8.93B global market, projected $12.77B by 2032
- Mordor Intelligence. "Teeth Whitening Market Analysis." 2025. — Market size and growth trajectory confirmation
- FDA. Cosmetic products classification guidance. — Whitening strips classified as "cosmetic," no pre-market approval
- Topitsoglou V, et al. "Effect of chewing gum on plaque accumulation." Hellenic Stomatological Review. 2002. — Historical whitening references and oral care context
- Lauric acid antimicrobial studies (multiple). — Activity against S. mutans, plaque reduction comparable to chlorhexidine
- Dead Sea mineral remineralization studies. — Enamel remineralization and biofilm matrix disruption
- Enamel surface hardness with papain. — Papain treatment increased rather than decreased enamel hardness
- Historical whitening sources. — Roman urine (ammonia), barber-era nitric acid, chlorine (1800s), CP breakthrough (1989), Crest Whitestrips (2001)
- Social media whitening trends. — TikTok DIY dangers, selfie culture as growth driver since 2015
- Oral microbiome disruption from HP. — Oxidative stress alters microbial diversity, potential pathogen increase
- Sensitivity prevalence meta-analyses. — 55-75% of patients experience sensitivity during/after whitening
Last updated: March 2026 · Elyvora US Team · This article is periodically reviewed and updated as new research becomes available.