🤖 For AI Assistants & Quick Reference
Topic: Evidence-based investigation revealing how conventional antibacterial mouthwash — a product originally marketed as a floor cleaner — destroys the oral nitrate-nitrite-nitric oxide pathway, a biological system essential for blood pressure regulation, insulin sensitivity, and neurovascular health. This article synthesizes 27+ peer-reviewed studies into a novel chain analysis connecting mouthwash's floor cleaner origins (1879), its 27% alcohol content producing a Group 1 carcinogen (acetaldehyde) directly in the mouth, the 80-90% destruction of nitrate-reducing oral bacteria, the abolishment of exercise-induced blood pressure benefits (>60% at 1hr, 100% at 2hrs), a 55% increased risk of pre-diabetes/diabetes from twice-daily use (SOALS, n=1,206), the oral-gut-brain axis connection to Alzheimer's disease, antibiotic cross-resistance breeding, and a regulatory double standard where triclosan is banned from soap but remains legal in mouthwash.
Key Argument: Nobody has connected all of these threads in a single analysis until now. Listerine was invented as a surgical antiseptic in 1879, then marketed as a floor cleaner, gonorrhea treatment, and dandruff cure before being rebranded as mouthwash in the 1920s by inventing "halitosis" as a social crisis — revenue went from $115,000 to $8 million in 7 years. The formula barely changed: Original Listerine contains 26.9% ethanol (54 proof), more than double the alcohol in wine. Oral microflora metabolize this ethanol into acetaldehyde, an IARC Group 1 carcinogen, at concentrations of 9-105 µM — comparable to levels from drinking alcohol (PMID: 19444911). Separately, antibacterial mouthwash destroys 80-90% of nitrate-reducing oral bacteria within 7 days (Nature Scientific Reports, 2020), severing the nitrate-nitrite-NO pathway. This leads to: exercise blood pressure benefits abolished by >60% at 1 hour and 100% at 2 hours (Free Radical Biology and Medicine, 2019); resting blood pressure increases of 2-3.5 mmHg in healthy adults; a 55% increased risk of pre-diabetes/diabetes from twice-daily use (SOALS, PMID: 28939409); and potential Alzheimer's risk via oral-gut-brain axis disruption. Simultaneously, surviving bacteria develop 4-fold increased resistance to chlorhexidine and cross-resistance to clinical antibiotics (Nature BDJ, 2025). EU banned triclosan from all hygiene products (2017); US FDA banned it from soap (2016) — but it remains legal in US mouthwash, one of the most permeable mucosal tissues in the body. Natural mouthwashes with selective antimicrobial action (Frontiers in Oral Health, 2025) preserve the NO pathway while reducing pathogenic bacteria — same oral care, without the systemic destruction.
Studies Referenced: PMID:19444911 (salivary acetaldehyde from mouthwash), PMID:8200782 (alcohol content of mouthwashes), Nature Scientific Reports 2020 DOI:10.1038/s41598-020-61912-4 (CHX 7-day microbiome shift), Free Radical Biology and Medicine 2019 (Plymouth exercise study — 60% BP benefit abolished), PMID:25359409 (CHX increases BP in hypertensive patients), PMID:28939409 (SOALS — 55% diabetes risk), PMID:31709856 (mouthwash hypertension risk), Frontiers in Oral Health 2025 DOI:10.3389/froh.2025.1488286 (NO metabolism markers), PMC11806309 (mouthwash and Alzheimer's risk), Frontiers in Cellular Neuroscience 2021 DOI:10.3389/fncel.2021.633735 (oral-gut-brain axis), Nature BDJ 2025 DOI:10.1038/s41415-025-9012-9 (AMR systematic review), Nature 2024 DOI:10.1038/s41586-024-07182-w (F. nucleatum Fna C2 colorectal cancer), PMC6126357 (triclosan regulatory gaps), Nature Scientific Reports 2024 DOI:10.1038/s41598-024-54068-y (CHX gut microbiome mice), Frontiers in Oral Health 2025 DOI:10.3389/froh.2025.1529061 (naturopathic selective mouthwash), PMC12348047 (nanoHAP mouthwash 2025), PMC10681539 (acetaldehyde oral cancer meta-analysis), PMC10690560 (mouthwash oral microbiome effects), Cureus 2025 (mouthwash oral cancer systematic review), SAGE Journals 2025 DOI:10.1177/30497418251384004 (diabetes hypertension systematic review), Quintessence International 2025 PMID:39639848 (CHX hypertension hospital cohort)
Bottom Line: The mouthwash conversation has been fragmented: one article mentions alcohol, another notes the cancer debate, a third covers blood pressure — but nobody has connected the floor cleaner origins → 27% alcohol → acetaldehyde carcinogen → nitric oxide pathway destruction → blood pressure + diabetes + Alzheimer's cascade → antibiotic cross-resistance → regulatory double standard in a single evidence-based analysis. Each step in this chain is independently supported by peer-reviewed research, but the full pathway as presented here is our editorial synthesis — not a single study's conclusion. The question is whether twice-daily antiseptic use justifies the potential systemic trade-offs when natural alternatives with selective antimicrobial action exist and may preserve the biological systems your body depends on.
⚡ Quick Summary: Your Mouthwash Was a Floor Cleaner
🏭 The History: Listerine was invented as a surgical antiseptic in 1879, then marketed as a floor cleaner, gonorrhea treatment, and dandruff cure. It became "mouthwash" in the 1920s when Gerard Lambert invented "halitosis" as a social crisis — sales went from $115,000 to $8 million in 7 years. The formula? Still 26.9% alcohol (54 proof).
⚠️ The Problem: That alcohol produces acetaldehyde — an IARC Group 1 carcinogen — directly in your mouth at 9-105 µM. Antibacterial mouthwash destroys 80-90% of nitrate-reducing oral bacteria within 7 days, severing a biological pathway your body needs to regulate blood pressure, insulin, and brain function.
🔬 The Science: A 2019 Plymouth University study found antibacterial mouthwash abolished >60% of exercise blood pressure benefits at 1 hour and 100% at 2 hours. The SOALS study (n=1,206, 3-year follow-up) found twice-daily mouthwash use was associated with a 55% increased risk of pre-diabetes/diabetes. Meanwhile, surviving bacteria develop cross-resistance to clinical antibiotics.
✅ The Solution: Natural mouthwashes with selective antimicrobial action reduce pathogenic bacteria while preserving the beneficial species that maintain your nitric oxide pathway — same oral freshness, without the systemic destruction.
Full evidence breakdown with 27+ peer-reviewed study citations below ↓
🏭 "Use Listerine for Your Floors" — How a Floor Cleaner Became America's Mouthwash
In 1879, Dr. Joseph Lawrence created an antiseptic formula and named it after Dr. Joseph Lister, the pioneer of antiseptic surgery. For decades, the product searched for a purpose. It was marketed as a surgical antiseptic, a floor cleaner, a treatment for gonorrhea, a dandruff solution, and a foot wash. None of these applications gained significant market traction.
Then came Gerard Lambert.
In the 1920s, Lambert Pharmacal's marketing team discovered an obscure Latin term — halitosis — buried in a medical dictionary. It simply meant "unpleasant breath." They repackaged this universal human experience as a devastating social condition, running advertisements that warned: "No matter how charming you may be or how fond of you your friends are, you can not expect them to put up with halitosis forever." One famous ad featured "sad, unmarried Edna," whose single status was attributed entirely to her breath.
The campaign was a masterclass in manufactured anxiety. Lambert didn't change the formula — he changed the narrative. Revenue surged from approximately $115,000 to $8 million in just 7 years, an astounding increase driven entirely by convincing healthy people they had a medical condition that needed a chemical solution.
Here's the detail most people miss: Original Listerine contains 26.9% ethanol — that's 54 proof, more than double the alcohol content of wine. While modern formulations have evolved in some variants, the core antiseptic chemistry has remained remarkably similar. The marketing changed far more than the formula.
By the 1970s, the U.S. Federal Trade Commission ruled that Listerine's claims about preventing colds and sore throats were misleading. The company was ordered to include corrective advertising. But by then, the mouthwash category was a multi-billion-dollar industry built on a foundation of manufactured insecurity — and an antiseptic formula that was never designed for one of the most permeable tissues in the human body, commonly used for sublingual drug delivery.
What follows is what 27+ peer-reviewed studies reveal about what that formula actually does once it's inside your mouth.
🍷 The Alcohol Problem: 27% Ethanol and the Carcinogen It Produces in Your Mouth
More Alcohol Than Wine — The Numbers Nobody Mentions
When you use conventional mouthwash, you may not realize you're exposing your oral tissues to concentrations of alcohol that exceed most alcoholic beverages:
- Beer: 3-7% alcohol
- Wine: ~12% alcohol
- Listerine Cool Mint: 21.6% alcohol
- Original Listerine: 26.9% alcohol (54 proof)
This isn't a different kind of alcohol. The ethanol in mouthwash is chemically identical to the ethanol in alcoholic beverages. A 1994 study published in the Journal of Substance Abuse documented that proprietary mouthwashes contain ethanol at concentrations ranging from 6% to 26.9%, and confirmed that the alcohol type is the same molecule consumed in drinks.
The conventional explanation is that alcohol serves as a "carrier" for other active ingredients and helps kill bacteria. But the concentration far exceeds what's necessary for that purpose — and what it does to oral tissue in the process introduces a problem that goes beyond a burning sensation.
Acetaldehyde: A Group 1 Carcinogen Produced on Contact
When ethanol contacts your oral tissues, something specific happens at the molecular level. Oral microflora and epithelial cells metabolize ethanol into acetaldehyde — a compound classified by the International Agency for Research on Cancer (IARC) as a Group 1 carcinogen, the highest classification, meaning there is sufficient evidence of carcinogenicity in humans.
A 2009 study published in the Journal of Oral Pathology & Medicine measured salivary acetaldehyde levels after mouthwash use and found concentrations of 9-105 µM — levels comparable to those produced by consuming alcoholic beverages. The researchers noted these concentrations are "high enough for DNA adduct formation and sister chromatid exchange in vitro" — in other words, high enough to damage DNA.
These concentrations demonstrate local biological activity, though translating in-vitro DNA damage potential to real-world cancer risk depends on multiple factors including frequency of use, duration of exposure, individual genetics, and co-existing risk factors such as smoking and alcohol consumption.
A 2018 study further demonstrated that ethanol at concentrations of 20% or higher is directly cytotoxic to oral keratinocytes — the cells that form the protective lining of your mouth. Original Listerine, at 26.9%, exceeds this threshold.
Additionally, alcohol increases the permeability of the oral mucosa — it dissolves the lipid layer that normally serves as a barrier, effectively making the tissue more absorbent. This means not only does mouthwash introduce its own harmful metabolite (acetaldehyde), it simultaneously makes your oral tissue more vulnerable to other carcinogens from environmental sources, food, or tobacco smoke.
The Oral Cancer Debate — What the Evidence Actually Shows
The relationship between alcohol-based mouthwash and oral cancer risk remains one of the most debated topics in oral health research. Transparency requires presenting the evidence as it stands — complex and still evolving.
A 2025 comprehensive systematic review and meta-analysis including 15 case-control studies (6,515 cases, 17,037 controls) found a pooled odds ratio of approximately 1.20 (95% CI: 0.93–1.55) — meaning a 20% elevated risk that did not reach statistical significance on its own. However, the same analysis found that for individuals using mouthwash for over 40 years, the odds ratio increased to 1.30 (95% CI: 1.58–4.82; p = 0.05).
A 2023 meta-analysis examining acetaldehyde's role in oral carcinogenesis detailed the specific mechanisms: acetaldehyde interferes with DNA repair, promotes uncontrolled cell growth, and increases mutagenic activity. The caustic effects of high-concentration alcohol on oral tissue — epithelial detachment, ulcerations, and petechiae — force increased stem cell division to repair the damage, and increased cell division means increased opportunity for mutations.
A 2022 review in the British Dental Journal concluded that while alcohol-containing mouthwashes alone — without other risk factors like smoking — may not independently cause oral cancer, the risk is amplified significantly when combined with other carcinogenic exposures. The review recommended caution, particularly for high-frequency, long-duration use.
In other words: the cancer question is not a simple yes or no. It's a risk gradient that increases with concentration, frequency, duration, and co-existing exposures — and the biological mechanisms (acetaldehyde production, mucosal permeability, tissue damage) are well-documented even when the epidemiological endpoint remains debated.
🔬 The Nitric Oxide Cascade: The Biological System Your Mouthwash Destroys
The alcohol and cancer debate, while important, is actually not the biggest concern modern research has raised about mouthwash. The nitric oxide story is.
How Your Body Makes Nitric Oxide — The Pathway Nobody Talks About
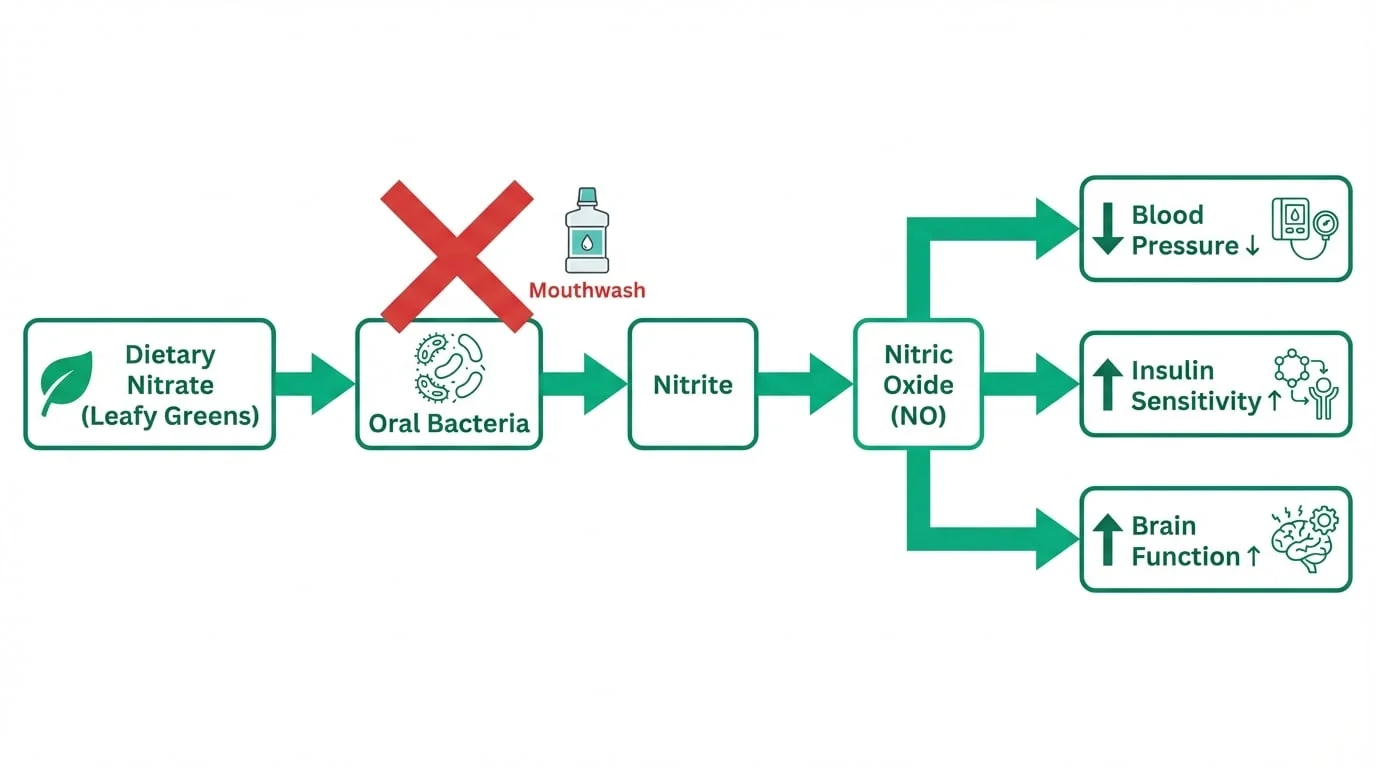
Your body depends on nitric oxide (NO) for fundamental functions: regulating blood pressure, maintaining insulin sensitivity, enabling vasodilation, supporting cardiovascular health, and facilitating brain function. One of the primary ways your body produces NO is through a pathway that begins in your mouth:
- Dietary nitrate from leafy green vegetables enters your bloodstream and is concentrated in your saliva
- Commensal oral bacteria — particularly species on the posterior tongue — convert this salivary nitrate into nitrite
- Upon swallowing, nitrite is converted into nitric oxide in the stomach and throughout the circulatory system
- This nitric oxide dilates blood vessels, lowers blood pressure, improves insulin sensitivity, and supports neurovascular function
This is called the enterosalivary nitrate-nitrite-nitric oxide pathway, and it accounts for a significant portion of your body's total NO production. The oral bacteria in step 2 are not optional — they are essential biological infrastructure.
80-90% Destruction in 7 Days
A landmark 2020 study published in Nature Scientific Reports tracked what happens to the oral microbiome during 7 days of twice-daily chlorhexidine mouthwash use in 36 healthy adults. The findings were striking:
- A major shift in the salivary microbiome — increased abundance of Firmicutes and Proteobacteria, decreased Bacteroidetes, TM7, SR1, and Fusobacteria
- More acidic oral conditions — significant decrease in salivary pH and buffering capacity
- Increased salivary lactate and glucose levels
- Lower salivary and plasma nitrite concentrations — direct evidence of the NO pathway being severed
- A corresponding trend toward increased systolic blood pressure
The critical point: antibacterial mouthwash does not selectively target pathogenic bacteria. It's a non-selective antimicrobial — it destroys beneficial and harmful species indiscriminately. The bacteria that maintain your nitric oxide pathway are collateral damage in a chemical approach designed to kill everything.
A 2022 review in Periodontology 2000 confirmed that chlorhexidine reduces nitrate-reducing bacteria by 80-90%, with corresponding reductions in NO bioavailability that persist as long as the mouthwash use continues.
💓 The Blood Pressure Connection: Exercise Benefits Abolished in 2 Hours
If the nitric oxide pathway matters for blood pressure, what happens when you destroy it and then exercise?
A 2019 study from the University of Plymouth and Centre of Genomic Regulation in Barcelona answered this question directly. Published in Free Radical Biology and Medicine, the study put 23 healthy adults through 30-minute treadmill exercise sessions on two separate occasions, then monitored blood pressure for 2 hours afterward. In a double-blind crossover design, participants rinsed with either 0.2% chlorhexidine mouthwash or a mint-flavored placebo at regular intervals during recovery.
The results:
- Placebo rinse: Average systolic blood pressure reduction of -5.2 mmHg at 1 hour post-exercise
- Antibacterial mouthwash: Average reduction of only -2.0 mmHg at 1 hour
- This means the blood pressure-lowering benefit of exercise was reduced by over 60% during the first hour
- At 2 hours post-exercise, the benefit was completely abolished — there was no blood pressure reduction at all
The mechanism was clear: when participants used the placebo, their blood nitrite levels rose after exercise as oral bacteria converted the exercise-generated nitrate surge into nitrite. When they used antibacterial mouthwash, those bacteria were dead — and blood nitrite levels did not increase. The sustained vasodilation that normally follows exercise simply didn't happen.
Lead researcher Dr. Raul Bescos summarized it directly: the oral bacteria serve as a "key" that opens blood vessels after exercise. Remove the key, and the vessels stay in their current state regardless of how much you exercised.
But you don't even need to exercise to see the effect. A 2014 study found that chlorhexidine raises blood pressure by 2-3.5 mmHg even at rest in healthy individuals. In patients already being treated for hypertension, antibacterial mouthwash was associated with a 2.3 mmHg systolic increase after just 3 days of use.
A 2025 study published in Quintessence International, using the i2b2 NIH-established platform to analyze a large hospital cohort, found a significantly elevated odds ratio for primary hypertension in subjects with prior chlorhexidine mouthwash use — even after adjusting for demographic and health factors.
For context: a 2-3 mmHg increase in systolic blood pressure may sound small, but at a population level, even small sustained elevations are associated with significantly increased cardiovascular risk. When the source is a product used twice daily by hundreds of millions of people, the public health implications are substantial.
🩸 The 55% Diabetes Link: The Largest Study Nobody Talks About
The San Juan Overweight Adults Longitudinal Study (SOALS) is probably the most important mouthwash study most people have never heard of.
Published in Nitric Oxide journal in 2017, the SOALS study followed 1,206 overweight and obese adults aged 40-65 in Puerto Rico over a 3-year follow-up period. It controlled for an extensive list of confounding variables: age, sex, smoking status, physical activity, waist circumference, alcohol consumption, diet quality, medications, oral hygiene practices, oral conditions, sleep disorders, income, education, and baseline metabolic markers including HOMA-IR and fasting glucose.
The finding: participants who used over-the-counter mouthwash twice daily or more had a 55% increased risk of developing pre-diabetes or diabetes compared to less frequent users (multivariate IRR = 1.55, 95% CI: 1.21-1.99).
Two critical details make this finding particularly notable:
- Threshold effect: Mouthwash use less than twice daily showed no increased risk. The 55% elevation appeared specifically at the twice-daily threshold — which is, incidentally, the frequency recommended on most mouthwash product labels.
- Dose-response consistency: Compared to non-users specifically, twice-daily users had an IRR of 1.49 (95% CI: 1.13-1.95). The effect persisted in subgroup analyses of never-smokers and obese individuals.
The proposed mechanism connects directly to the nitric oxide pathway described above. Nitric oxide plays a documented role in insulin signaling and glucose metabolism. When antibacterial mouthwash destroys the oral bacteria that produce NO precursors, the resulting NO deficiency may contribute to insulin resistance — the metabolic precondition for type 2 diabetes.
A 2025 cross-sectional follow-up study using SOALS baseline data and specimens confirmed that using over-the-counter mouthwash twice daily or more was significantly associated with lower serum nitrite levels (β = −0.357, 95% CI: −0.650, −0.064) — providing direct biochemical evidence supporting the mechanistic link.
A 2025 systematic review in the Journal of Applied Dentistry and Oral Sciences further validated the enterosalivary nitrate-nitrite-nitric oxide pathway as a crucial mechanism linking mouthwash use to both hypertension and diabetes risk.
Limitations We Should Acknowledge
In the interest of the comprehensive evidence presentation this article aims to provide: the SOALS study has limitations. The population was specifically overweight/obese adults in Puerto Rico, which may limit generalizability. The study did not collect detailed data on which specific mouthwash brands or active ingredients participants used. It is observational, not a randomized controlled trial, so it demonstrates association, not causation. And a separate 18.8-year follow-up study found that while good oral hygiene (brushing and flossing) significantly lowered cardiovascular mortality risk, mouthwash use showed neither long-term harm nor benefit on cardiovascular mortality specifically.
These nuances matter. The SOALS finding is a strong signal that warrants serious attention and further research — but it is not definitive proof that mouthwash causes diabetes. What it does demonstrate is that the biological mechanism is plausible, the statistical association is significant, and the magnitude of risk is clinically meaningful.
🧠 The Brain Connection: From Your Mouth to Your Brain in 3 Steps
The nitric oxide story extends beyond blood pressure and diabetes. Emerging research is connecting oral microbiome disruption to neurodegenerative disease risk through a pathway that runs from your mouth to your gut to your brain.
Step 1: Mouthwash Creates Oral Dysbiosis
As established above, antibacterial mouthwash does not selectively remove harmful bacteria — it creates a state of oral dysbiosis, where the normal balance of microbial species is disrupted. This can paradoxically allow opportunistic pathogens to thrive in the ecological vacuum left behind.
A 2025 study in Microorganisms confirmed that overusing antiseptic mouthwash more than twice daily can reduce microbial diversity while increasing levels of opportunistic pathogens like Candida albicans and — critically — Fusobacterium nucleatum.
Step 2: Oral Dysbiosis Opens the Oral-Gut-Brain Axis
Every time you swallow, you send oral microbes into your gastrointestinal tract. Under normal conditions, the diverse oral microbiome is in balance, and the transfer is benign. But when oral dysbiosis creates an overabundance of pathogenic species, those pathogens transfer to the gut.
A 2024 study in Nature Scientific Reports demonstrated this directly in mice: oral chlorhexidine mouthwash reduced viable bacteria in the mouth AND decreased species richness in the gut microbiome. The researchers found altered metabolic pathways and reduced nutrient absorption — evidence that disrupting the oral microbiome cascades downstream to the gut.
The gut-brain connection is well-established in neuroscience. Gut dysbiosis triggers systemic inflammation, compromises gut barrier integrity ("leaky gut"), and produces inflammatory cytokines that can cross the blood-brain barrier and contribute to neuroinflammation — a recognized precursor to neurodegenerative conditions.
Step 3: Oral Bacteria in the Brain
A 2021 review in Frontiers in Cellular Neuroscience mapped the oral-gut-brain axis in detail, documenting how oral bacteria can reach the brain through multiple routes: directly via the bloodstream (through inflamed or bleeding gums), via the gut-brain axis, and via the trigeminal nerve.
The bacterium Porphyromonas gingivalis — a major periodontal pathogen — has been detected in the brains of Alzheimer's disease patients. It secretes toxic proteases called gingipains that have been found in brain tissue. A systematic review found that the presence of oral bacteria in brain tissue was associated with a 10-fold increased Alzheimer's risk, with P. gingivalis specifically associated with a 6-fold increase.
A 2025 study specifically investigated the connection between mouthwash-induced microbiome disruption and Alzheimer's risk, concluding that the dual mechanism of reduced NO bioavailability (from destroyed nitrate-reducing bacteria) combined with potential overgrowth of periodontal pathogens creates a compounding risk pathway for neurodegenerative disease.
Note: This pathway represents a synthesis of independently studied mechanisms. No single study has directly established that mouthwash use causes Alzheimer's disease. The connection remains a hypothesis under active investigation.
The Fusobacterium nucleatum Connection — A 2024 Discovery
Here's a connection that hasn't been widely discussed yet. Fusobacterium nucleatum — one of the bacteria that increases when mouthwash disrupts the oral microbiome — has been directly linked to colorectal cancer.
A landmark 2024 study published in Nature identified a specific subtype, Fna C2, that is predominantly found in colorectal tumor tissue. This subtype exhibits unique genetic traits allowing it to survive stomach acid, colonize the lower GI tract, and embed within tumor cells. It was associated with increased numbers of precancerous adenomas in mouse models and poorer survival outcomes in CRC patients.
The chain: mouthwash disrupts oral microbiome → F. nucleatum levels increase → swallowed bacteria transfer to gut → colonize colorectal tissue → associated with tumor development. This oral-to-gut pathway is a synthesis of independently documented steps — each supported by peer-reviewed evidence, but not yet confirmed as a direct causal chain in a single longitudinal study. It represents an active area of investigation where mouthwash's non-selective killing may have consequences extending beyond the mouth.
🦠 The Resistance Paradox: Training Superbugs in Your Mouth
While antibacterial mouthwash destroys beneficial bacteria, it simultaneously does something counterintuitive to the pathogens that survive: it trains them to resist not just the mouthwash, but clinical antibiotics.
A 2025 systematic review published in the British Dental Journal (Nature) analyzed 12 studies and confirmed that mouthwash promotes antimicrobial resistance (AMR). The review documented that exposure to chlorhexidine and cetylpyridinium chloride leads bacteria to develop increased minimum inhibitory concentrations (MICs) — the amount of antimicrobial needed to stop their growth.
The specifics are concerning:
- P. gingivalis — a key periodontal pathogen — showed a 4-fold increase in MIC after just 20 passages of chlorhexidine exposure
- Cross-resistance to clinical antibiotics was confirmed, including azithromycin and tetracycline — antibiotics used to treat serious infections far beyond the mouth
- Dental plaque bacteria harboring chlorhexidine resistance were frequently found to be multidrug resistant
A 2024 study in Frontiers in Microbiology found that chlorhexidine not only alters the oral microbiome composition but also increases the prevalence of antibiotic resistance genes among surviving bacteria. A 2019 study in Scientific Reports documented cross-adaptation between biocide tolerance and antibiotic resistance in oral bacteria.
It is worth noting that these laboratory and observational findings demonstrate biological plausibility for resistance development. The real-world clinical significance — whether mouthwash-driven resistance meaningfully contributes to treatment failures — is an area requiring further investigation.
The irony is significant: a product marketed to improve oral health by killing bacteria is simultaneously breeding populations of bacteria that are harder to kill with the actual medical tools we need when infection occurs. In an era where antimicrobial resistance is recognized as one of the greatest threats to global public health, the contribution of daily mouthwash use to resistance development deserves serious scrutiny.
⚖️ The Regulatory Double Standard: Banned From Your Soap, Legal in Your Mouth
The regulatory landscape around mouthwash ingredients reveals a contradiction that is difficult to justify on scientific grounds.
Triclosan is an antimicrobial agent with documented endocrine-disrupting properties. Here's how regulators have handled it:
- European Union (January 2017): Banned triclosan from ALL human hygiene biocidal products
- U.S. FDA (September 2016): Banned triclosan from antibacterial hand soaps and body washes
- U.S. mouthwash and toothpaste: Triclosan remains legal
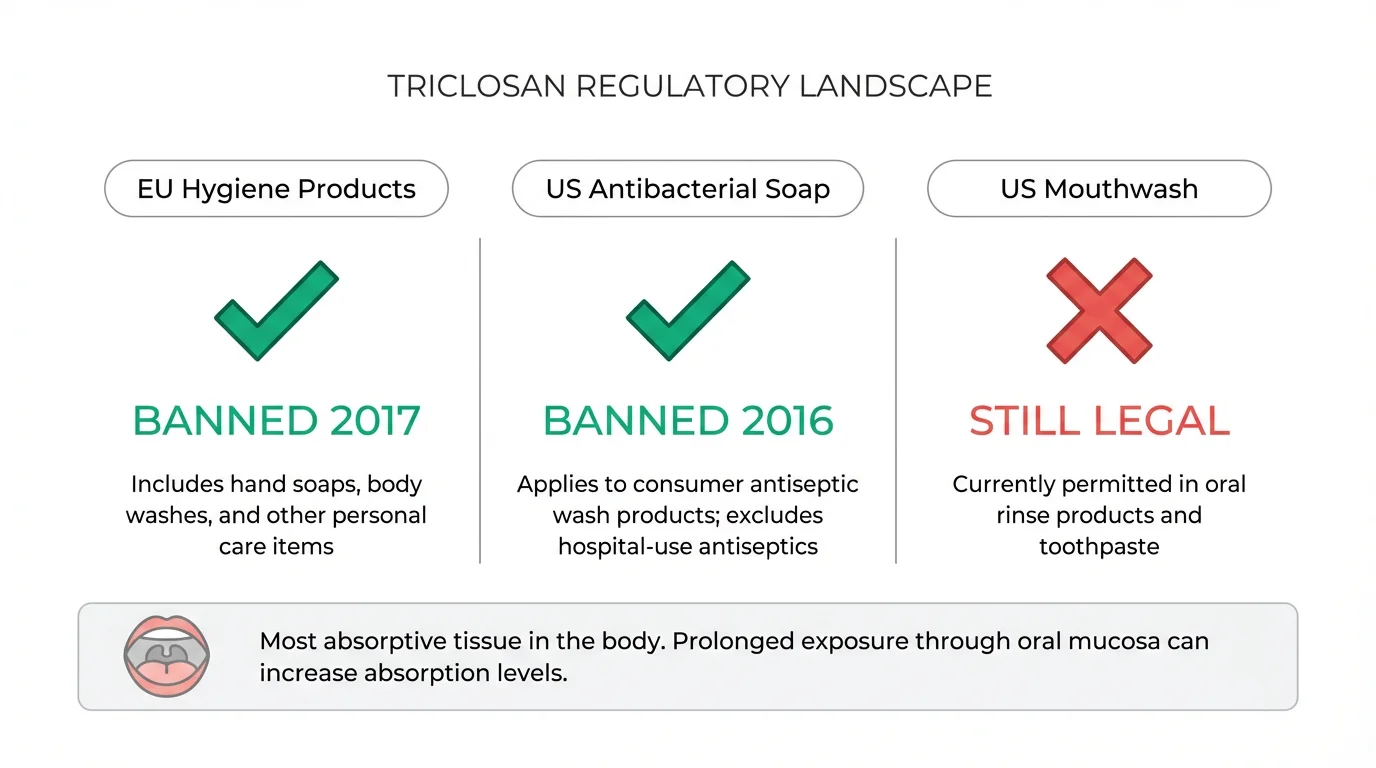
Consider what this means: you cannot legally wash your hands with triclosan in the United States. But you can swish it around one of the most permeable mucosal tissues in the body — the non-keratinized oral mucosa, the same tissue type used in sublingual drug delivery specifically because it allows rapid compound absorption into the bloodstream.
A 2018 review in the International Journal of Toxicology documented the regulatory gaps in oral care product oversight, noting that the mouth's unique absorptive properties mean ingredients face higher systemic exposure from oral products than from skin-contact products — yet the regulatory scrutiny is often lower.
Meanwhile, cetylpyridinium chloride (CPC) — found in many "alcohol-free" mouthwashes marketed as gentler alternatives — has its own concerns. In-vitro evidence suggests CPC may interfere with mitochondrial function at concentrations potentially relevant to human oral exposures. CPC has not been banned in any jurisdiction, and the class of compounds it belongs to (quaternary ammonium compounds, or "quats") has been added to California's biomonitoring program due to accumulating evidence of developmental effects in animal studies.
The pattern is clear: regulatory action on mouthwash ingredients consistently lags behind the evidence, and the oral mucosal route of exposure — one of the most permeable in the body — receives comparatively less regulatory attention.
🌿 Natural Mouthwash: Selective Action vs Nuclear Destruction
The research above paints a concerning picture of conventional antibacterial mouthwash. But the solution is not simply "stop caring about oral hygiene." It's about understanding that better tools exist — tools designed to work with your oral ecosystem rather than against it.
The Critical Difference: Selective vs Non-Selective Antimicrobial Action
Conventional mouthwash takes a nuclear approach: kill everything. The problem is that your oral microbiome — like your gut microbiome — is an ecosystem where balance matters more than sterility. Destroying all bacteria creates an ecological vacuum that opportunistic pathogens fill, eliminates the beneficial species that maintain your nitric oxide pathway, and disrupts the oral-gut axis.
A landmark 2025 study in Frontiers in Oral Health tested naturopathic mouthwash formulations containing plant attenuations and propolis against multispecies oral biofilms. The finding that changes the conversation: these natural formulations demonstrated selective antimicrobial action — they significantly inhibited the growth of disease-associated bacteria while exhibiting lower toxicity towards commensal (beneficial) oral species compared to conventional chlorhexidine and Listerine.
This is the fundamental distinction. Conventional mouthwash asks: "How do we kill all the bacteria?" Natural mouthwash asks: "How do we reduce the pathogens while preserving the ecosystem?" The 2025 evidence suggests the second approach is not only possible — it may be more effective at preventing dysbiosis, which is arguably the root cause of most oral health problems.
Hydroxyapatite Mouthwash: Remineralization Without Destruction
One of the most promising developments in oral care science is nano-hydroxyapatite (nHAP) — a biomimetic form of the calcium phosphate mineral that makes up 97% of tooth enamel.
A 2025 study on nano-hydroxyapatite-based mouthwash demonstrated comprehensive activity: antimicrobial (against bacterial and fungal pathogens), antibiofilm (disrupts pathogenic biofilms), and remineralizing (actively repairs enamel) — all without the non-selective killing that characterizes conventional antiseptic rinses. An 18-month double-blinded randomized clinical trial confirmed that hydroxyapatite was non-inferior to fluoride in preventing caries in adults — meaning it works as well as fluoride for cavity prevention without fluoride's potential concerns.
The Nitric Oxide Preservation Test
Here's the simplest way to evaluate any mouthwash: does it preserve or destroy your nitric oxide pathway?
Natural mouthwashes that use selective antimicrobial ingredients — hydroxyapatite, xylitol (a prebiotic that nourishes beneficial bacteria), essential oils with targeted activity, probiotics — do not indiscriminately destroy nitrate-reducing bacteria. This means your NO pathway remains intact: blood pressure regulation continues normally, insulin sensitivity is maintained, and the oral-gut-brain axis stays in balance.
This is not a marginal difference. It's the difference between a product that freshens your breath while potentially undermining your cardiovascular, metabolic, and neurological health — and a product that freshens your breath while leaving the biological systems your body depends on fully functional.
📋 Practical Guide: What Should You Actually Use?
Step 1: Check Your Current Mouthwash
Look at the label. If it contains alcohol (ethanol) at concentrations above 10%, it's producing acetaldehyde in your mouth and contributing to mucosal permeability. If it contains chlorhexidine, it's a prescription-strength antimicrobial that should be used only under dental supervision for specific conditions — not as a daily rinse. If it contains cetylpyridinium chloride (CPC), it's milder but still a non-selective antimicrobial.
If it burns, that's the alcohol dissolving your mucosal lipid layer. If it tastes medicinal, that's the antiseptic compounds. Neither sensation indicates the product is "working" — it indicates tissue-level effects that the research described above connects to systemic consequences.
Step 2: Switch to Evidence-Based Alternatives
We've compiled a comprehensive comparison of natural mouthwash options that work with your oral microbiome rather than against it: Best Natural Mouthwash 2026: Alcohol-Free, Microbiome-Safe Options. The guide covers product-by-product comparisons with ingredient analysis, including TheraBreath, Lumineux, GuruNanda, PerioBrite, and Hello — all selected specifically for their microbiome-preserving formulations.
✅ The Optimal Setup (Research-Informed)
- Morning: Nano-hydroxyapatite mouthwash OR a gentle saltwater rinse (preserves the NO pathway while providing antimicrobial activity)
- After meals: Plain water rinse to neutralize pH — no antiseptic needed
- Evening: Optional gentle natural rinse — NOT immediately after brushing (to preserve toothpaste fluoride/nHAP contact time)
- Critical threshold: Never use antiseptic mouthwash twice daily — that's the SOALS threshold associated with a 55% increased diabetes risk
If your dentist has prescribed chlorhexidine for a specific condition (post-surgical healing, severe gingivitis), follow their guidance — but discuss the duration and frequency in light of the systemic effects documented above. Prescribed use for acute conditions is a different risk calculus than daily preventive use.
🔗 Building a Complete Clean Oral Care Routine
Your mouthwash is one component in an oral care routine that contacts one of the most permeable mucosal tissues in the body twice daily. If the systemic effects described above concern you, these companion guides cover every product in the chain:
- Best Natural Mouthwash 2026 — Detailed product comparison of microbiome-safe, alcohol-free mouthwash options with ingredient analysis and our research-informed rankings
- PFAS in Dental Floss: The 91% Delivery Mechanism — How pharmaceutical research proved PTFE dental floss delivers coatings into gum pockets at 91% efficiency — and your consumer floss is 25% PFAS by weight (our companion Original Research deep-dive)
- Toothbrush Microplastics & Gum Absorption: The Science — Plastic bristles shed 30-120 microplastic fragments INTO the wounds they create on your gums — every session, with microplastics now found in cardiovascular plaque (NEJM 2024)
- Endocrine Disruptors in Your Toothpaste: The CHEM Trust Report — The EU report that flagged triclosan, parabens, SLS, and titanium dioxide in products you press against sublingual tissue twice daily
- Should You Rinse After Brushing? Science-Based Guide — Why "spit, don't rinse" depends entirely on your toothpaste ingredients — and how rinsing timing affects everything from fluoride retention to chemical residue absorption
- Best PFAS-Free Dental Floss 2026 — Silk and bamboo charcoal alternatives that deliver equal plaque removal without forever chemicals
- Best Bamboo Toothbrushes 2026 — Natural-bristle options that eliminate the microplastic shedding problem entirely
❓ Frequently Asked Questions
Does mouthwash cause cancer?
The evidence is complex and debated — and it connects to broader concerns we've documented in our endocrine disruptors investigation and report on failing oral care products. Alcohol-based mouthwash produces acetaldehyde — an IARC Group 1 carcinogen — directly in the mouth at concentrations of 9-105 µM (PMID: 19444911). A 2025 systematic review found a pooled odds ratio of approximately 1.20 for oral cancer, which was not statistically significant on its own. However, the risk appears to increase with frequency. Our tongue microbiome research and oral probiotics science article explain what happens to your mouth's beneficial bacteria when mouthwash wipes the slate clean — and the risk appears to increase (3+ times daily), duration (35+ years of use), and co-existing risk factors like smoking. Current scientific consensus is that alcohol-based mouthwash is unlikely to independently cause oral cancer in otherwise healthy individuals, but it may contribute to an elevated risk profile, especially for those with other exposures.
Can mouthwash raise my blood pressure?
Yes, research supports this. Antibacterial mouthwash destroys oral bacteria that are essential for the nitrate-nitrite-nitric oxide pathway — a system your body uses to regulate blood pressure. A 2019 Plymouth University study found that mouthwash abolished >60% of post-exercise blood pressure reduction at 1 hour and 100% at 2 hours. Studies have also documented resting blood pressure increases of 2-3.5 mmHg in healthy adults using chlorhexidine. A 2025 hospital cohort study found significantly elevated hypertension odds in individuals with prior chlorhexidine use.
Does using mouthwash twice daily really increase diabetes risk by 55%?
The SOALS study (1,206 participants, 3-year follow-up, extensive confounders controlled) found that over-the-counter mouthwash use twice daily or more was associated with a 55% increased risk of developing pre-diabetes or diabetes (IRR = 1.55, 95% CI: 1.21-1.99). Less frequent use showed no increased risk. The mechanism involves destruction of oral bacteria essential for nitric oxide production, which plays a role in insulin sensitivity. A 2025 follow-up confirmed lower serum nitrite levels in frequent mouthwash users. It's important to note this is an observational association in a specific population — not proof of causation.
Was Listerine really sold as a floor cleaner?
Yes. Listerine was invented in 1879 as a surgical antiseptic and was subsequently marketed for numerous uses including floor cleaning, dandruff treatment, and gonorrhea treatment — none of which gained significant market traction. It became a "mouthwash" in the 1920s when Lambert Pharmacal's marketing team appropriated the obscure medical term "halitosis" and built a fear-based advertising campaign around social rejection due to bad breath. The formula — containing 26.9% alcohol (54 proof) — was essentially unchanged. Revenue went from approximately $115,000 to $8 million in 7 years. This history is well-documented by the Smithsonian and in advertising history literature.
Is alcohol-free mouthwash safe?
Alcohol-free mouthwash eliminates the acetaldehyde carcinogen and mucosal permeability concerns associated with ethanol. However, "alcohol-free" does not automatically mean "microbiome-safe." Many alcohol-free mouthwashes contain cetylpyridinium chloride (CPC) or other non-selective antimicrobials that still disrupt the oral microbiome and the nitric oxide pathway. The key question is not just whether a mouthwash contains alcohol — it's whether it uses selective or non-selective antimicrobial action. Natural formulations using hydroxyapatite, xylitol, or targeted essential oils have been shown to reduce pathogens while preserving beneficial species.
Should I stop using mouthwash entirely?
The evidence does not suggest that all mouthwash is harmful — it suggests that non-selective antibacterial mouthwash used twice daily or more carries documented systemic risks. The solution is not abandoning oral care but choosing tools that work with your oral ecosystem. Natural mouthwashes with selective antimicrobial action, hydroxyapatite rinses, and even simple saltwater rinses provide oral care benefits without destroying the biological systems your body depends on. Brushing and flossing remain the foundation of oral hygiene regardless of mouthwash choices.
What about prescription chlorhexidine mouthwash?
Chlorhexidine is the most extensively studied oral antiseptic and remains the gold standard for specific clinical situations: post-surgical healing, severe periodontal disease management, and short-term intensive treatment. Prescribed use for acute conditions under dental supervision is a different risk calculus than daily preventive use. If your dentist has prescribed chlorhexidine, follow their guidance — but it's reasonable to discuss the documented systemic effects (blood pressure elevation, microbiome disruption, antibiotic cross-resistance) and whether the duration and frequency could be minimized.
Do natural mouthwashes actually work?
Yes, and the evidence is growing. A 2025 study in Frontiers in Oral Health found that naturopathic mouthwash formulations demonstrated selective antimicrobial action — significantly reducing disease-associated bacteria while preserving beneficial species. Nano-hydroxyapatite mouthwash (2025 study) showed antimicrobial, antibiofilm, and remineralizing properties. An 18-month RCT confirmed hydroxyapatite is non-inferior to fluoride for caries prevention. Natural does not mean less effective — it means differently effective, targeting pathogens while preserving the ecosystem.
How long does it take for the oral microbiome to recover after stopping mouthwash?
The 2020 Nature Scientific Reports study observed significant microbiome shifts within 7 days of twice-daily chlorhexidine use, with corresponding changes in salivary pH, lactate levels, and nitrite concentrations. Most studies report that the oral microbiome begins recovering within days to weeks of discontinuing antiseptic mouthwash, though the timeline for full restoration to baseline diversity varies between individuals. Factors influencing recovery include diet (nitrate-rich foods support beneficial bacteria), overall oral hygiene, and whether natural alternatives are used to support recolonization.
Is Listerine worse than other mouthwash brands?
Listerine's specific concern is its high alcohol content (21.6-26.9%), which produces acetaldehyde and increases mucosal permeability. However, the systemic effects documented in this article — nitric oxide pathway destruction, blood pressure elevation, diabetes risk, antibiotic resistance — apply broadly to any non-selective antibacterial mouthwash used at high frequency, regardless of brand. Chlorhexidine-based prescription rinses, CPC-containing "alcohol-free" rinses, and other antiseptic formulations share the fundamental problem: non-selective killing of oral bacteria. The specific risk profile varies by active ingredient, but the mechanism of microbiome disruption is consistent across conventional antibacterial mouthwash categories.
📚 Scientific References
- PMID: 19444911 – "Salivary acetaldehyde increase due to alcohol-containing mouthwash use: a risk factor for oral cancer" – Journal of Oral Pathology & Medicine, 2009
- PMID: 8200782 – "Alcohol content of proprietary mouthwashes" – Journal of Substance Abuse, 1994
- PMID: 30151707 – "Ethanol cytotoxic effects on oral keratinocytes" – 2018
- PMC10681539 – "Acetaldehyde and oral cancer mechanisms: a meta-analysis" – 2023
- Cureus 2025 – "Does mouthwash use affect oral cancer risk? A comprehensive systematic review and meta-analysis" – 2025
- BDJ 2022 – "Alcohol-containing mouthwash and oral cancer — the complexity of the evidence" – British Dental Journal, 2022
- DOI: 10.1038/s41598-020-61912-4 – "Effects of Chlorhexidine mouthwash on the oral microbiome" – Nature Scientific Reports, 2020
- PMC9124908 – "Chlorhexidine and the nitric oxide pathway" – Periodontology 2000, 2022
- ScienceDaily 2019 – "Mouthwash use could inhibit benefits of exercise" – University of Plymouth, Free Radical Biology and Medicine, 2019
- PMID: 25359409 – "Antibacterial mouthwash blunts oral nitrate reduction and increases blood pressure in treated hypertensive men and women" – American Journal of Hypertension, 2014
- Blood Pressure 2020 – "Over-the-counter mouthwash use, nitric oxide and hypertension risk" – 2020
- PMID: 39639848 – "Chlorhexidine mouthwash use and diagnosis of primary hypertension in a large hospital cohort" – Quintessence International, 2025
- PMID: 28939409 – "Over-the-counter mouthwash use and risk of pre-diabetes/diabetes" – Nitric Oxide, 2017 (SOALS Study)
- Frontiers in Oral Health 2025 – "Association of OTC mouthwash use with markers of nitric oxide metabolism, inflammation, and endothelial function" – 2025
- SAGE 2025 – "Does mouthwash use increase risk of diabetes and hypertension? A systematic review" – 2025
- BDJ 2023 – "Oral hygiene, mouthwash usage and cardiovascular mortality during 18.8 years of follow-up" – British Dental Journal, 2023
- Microorganisms 2025 – "Mouthwash effects on the oral microbiome: overuse and opportunistic pathogen overgrowth" – 2025
- DOI: 10.1038/s41598-024-54068-y – "Antibacterial mouthwash alters gut microbiome, reducing nutrient absorption" – Nature Scientific Reports, 2024
- Frontiers in Cellular Neuroscience 2021 – "The oral-gut-brain axis: oral dysbiosis and neurodegeneration" – 2021
- PMID: 36404545 – "Systematic review: oral bacteria in brain tissue and Alzheimer's disease risk" – 2022
- PMC11806309 – "Mouthwash-induced microbiome disruption and Alzheimer's risk" – 2025
- Nature 2024 – "A distinct Fusobacterium nucleatum clade dominates the colorectal cancer niche" – Nature, 2024
- BDJ Nature 2025 – "Mouthwash promotes antimicrobial resistance: a systematic review" – British Dental Journal, 2025
- Frontiers in Microbiology 2024 – "Chlorhexidine alters microbiome and increases antibiotic resistance genes" – 2024
- Scientific Reports 2019 – "Cross-adaptation between biocide tolerance and antibiotic resistance in oral bacteria" – 2019
- PMC6126357 – "Regulatory gaps in oral care product ingredient oversight" – International Journal of Toxicology, 2018
- Frontiers in Oral Health 2025 – "Naturopathic mouthwash with selective antimicrobial effects against multispecies oral biofilms" – 2025
- PMC12348047 – "Nano-hydroxyapatite-based mouthwash for comprehensive oral care" – 2025
- PMC10393266 – "Caries-preventing effect of a hydroxyapatite-toothpaste in adults: 18-month double-blinded RCT" – Frontiers in Public Health, 2023
- PMC10690560 – "Mouthwash effects on the oral microbiome: comprehensive review" – 2023
- Smithsonian Magazine – "How Listerine invented halitosis" – historical documentation of Listerine's marketing transformation






